1.0 What is fibrillation?
Fibrillation is an arrhythmia that affects either the atria as a pair, or the ventricles as a pair, producing “a-fib”, or “v-fib”, respectively. Most cardiac rhythms are organized – they’re regular in some way, producing some sort of regular (as opposed to disorganized), rhythmic motion of the chambers, hopefully producing a blood pressure. In fibrillation, the cardiac tissue of the chambers involved wiggles about like (classic phrase) “a bag of worms”. Does a chamber wiggling like a bag of worms pump any blood, produce a cardiac output, eject any fraction of its contents? No, it does not!As I always try to point out, all the waves that you see on ECG strips actually represent some kind of physical motion of one or the other set of cardiac chambers, and the trick is to try to visualize what those chambers are doing in any given rhythm situation. Let’s see if a quick review of some strips helps the visualization process.
Here we are familiar Sinus rhythm on image 01. Organized, rhythmic, producing stable contraction of the chambers – first the atria, then the ventricles. So nice orderly motion, first above, then below.
 Image 01
Image 01
Next slide (Image ) atrial flutter. Still organized: the atria are contracting rapidly, sure, at about 300 bpm, and the ventricles are responding to every third or fourth impulse, slowly enough that the ventricular chambers have time to fill up nicely between beats, fast enough to probably maintain a good blood pressure. So I visualize the atria clipping along, with the ventricles contracting every third or fourth time.

Image 02
This one? Well – is it organized? Actually it is: see the pattern of doubles? It’s a little easier to figure out by looking at the lower part of the strip – this is a sinus rhythm, and after every sinus beat comes a PAC, followed by a compensatory pause. So yes, still organized. “Regularly irregular”.

Image 03 How about this one? , VT. Ugly, scary, but still organized, regular – the chambers (which ones?) are moving in a steady manner. On your mental screen you should see the ventricular walls contracting very rapidly – do they have time to fill? Should we shock this rhythm? It depends…

Image 04
1-1: What is atrial fibrillation
How about this one? Not organized? Should we shock this rhythm? A-fib for sure can be a shock able rhythm, but look at the QRS rate – in the 70’s. What would have to be happening to make this a shock able situation? What do you visualize here? Atria: bag of worms. Ventricles – occasional, but normally conducted QRS’s. Are they too slow or too fast to make a blood pressure? How do you tell?
 Image 05
Image 05
1-2: What is ventricular fibrillation?Here’s an ugly one - you probably recognize this one right off. Doesn’t look organized to me! What rhythm is this? Visualize the ventricles – everybody see the worms? What should we do?
 Image 06
Image 06
2- What is De-fibrillation?
So: all set on organized, and not organized? The treatment for nasty arrhythmia is often electrical, right? The point is: one type of treatment: cardioversion - is for the organized kind of rhythm, and the other is, De-fibrillation is for disorganized rhythms.
What you want to do is to send a fixed amount of electrical energy along the normal conduction path of the heart: along the Lead II pathway.
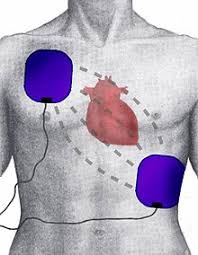
Image 07
Here’s a diagram of the normal lead II: the positive electrode is down near the apex of the ventricles, the negative one is at the atrial end. Everybody remembers that the normal direction that the cardiac impulse takes is from the SA node at the northwest corner, up near Oregon, down and towards the southeast in Florida, where the positive electrode lives? And that the signal moves along the pathway as the cells depolarize, in sequence, along that pathway?
2.0: What is a defibrillator.
 The goal here is to try to understand what the machine is trying to do. Let’s say your patient pops into a nasty rhythm – not handling it very well, not making much of a blood pressure; and you want to deliver electricity – what do you need?
The goal here is to try to understand what the machine is trying to do. Let’s say your patient pops into a nasty rhythm – not handling it very well, not making much of a blood pressure; and you want to deliver electricity – what do you need?
2.1: The monitor.
you need to be able to see what’s going on. This is of course one of the
reasons why our patients are monitored at the bedside: so you can see
what rhythm your patient is in. Defibrillators are built to travel– so they
have a built in monitor screen.
2.3: The capacitor.

Generally you need a battery to run any transportable medical device.
Due to rechargeable batteries these devices are so heavy. The batterystores electricity,when machine is plugged in to AC. The capacitor fills
up with electricity when you push the button that selects charge .
2.4: The paddles and the pads:
Paddles

Self Adhesive Pads
 Internal Paddles
Internal Paddles
paddles are considered “old-tech” – nowadays the thing to do is to slap on sticky defibrillation pads that hook up to the machine – the same ones as
external pacing pads – then stand back, charge and discharge the machine
from a few feet away. The shock can be delivered to the heart by means of
electrode placed on chest of the patient(External defibrillation) or the electrode
may be held directly against the heart when the chest is open
(internal defibrillation). Higher voltage are required for external defibrillation
than for internal defibrillation.
2.5: Theory of operation.
Schematic diagram of a defibrillator
Above schematic show basic circuit diagram of DC Defibrillator. A Variable auto transformer forms the primary of a high voltage transformer. The output voltage transformer is rectified by a diode rectifier and is connected to vacuum type high voltage change over switch. In position 1, the switch is connected to one end of an oil filled micro farad capacitor. In this position, the capacitor charge to a voltage set by the positioning of the auto transformer. When the shock is delivered to the patient, a foot switch or a push button mounted on the handle of the electrode is operated. The high voltage switch change over to position 2 and the capacitor is discharged across the heart through the electrode. The inductor in the circuit slow down the discharge from capacitor by induced counter voltage. This give the output pulse a physiologically favorable shape. The dis advantage of using inductor is that any practical inductor will have its own resistance and dissipates part of the energy during the discharge process. The shape of waveform that appears across electrodes will depend upon the value of the capacitor and inductor used in the circuit. The discharge resistance which the patient represent for defibrillating pulse may be regarded as purely ohmic resistance of 50-100 Ω approximately for typical electrode size of 80 cm2. The typical discharge pulse of defibrillator is shown in fig.3 b. Using this design, external defibrillation uses: –50 to 100 Joules of energy when electrodes are applied directly to the heart –Up to 400 Joules when applied externally ,Capacitors used range from 10 to 50F .Voltage using these capacitors and max energy (400J) ranges from 1 to 3 kV . Energy loss result in the delivery of less than theoretical energy to the heart
Defibrillator: Rectangular-Wave
•Capacitor is discharged through the subject by turning on a series silicon- controlled rectifier.
•When sufficient energy has been delivered to the subject, a shunt silicon- controlled rectifier short-circuits the capacitor and terminates the pulse, eliminating a long discharge tail of the waveform
•Output control can be obtained by varying:
–Voltage on the capacitor
–Duration of discharge
•Advantages of this design:
–Requires less peak current
–Requires no inductor
–Makes it possible to use physically smaller electrolytic capacitors
–Does not require relays ·

Monophasic pulse width is typically programmable from 3.0 to 12.0 msecBiphasic positive pulse width is typically programmable from 3.0 to 10.0 msec, while the negative pulse is from 1.0 to 10.0 msec ·
Studies suggest that biphasic pulses yield increased defibrillation efficacy with respect to Monophasic pulses.
Reference : http://coep.vlab.co.in
Ventricular Fibrillation
Fibrillation is an arrhythmia that affects either the atria as a pair, or the ventricles as a pair, producing “a-fib”, or “v-fib”, respectively. Most cardiac rhythms are organized – they’re regular in some way, producing some sort of regular (as opposed to disorganized), rhythmic motion of the chambers, hopefully producing a blood pressure. In fibrillation, the cardiac tissue of the chambers involved wiggles about like (classic phrase) “a bag of worms”. Does a chamber wiggling like a bag of worms pump any blood, produce a cardiac output, eject any fraction of its contents? No, it does not!As I always try to point out, all the waves that you see on ECG strips actually represent some kind of physical motion of one or the other set of cardiac chambers, and the trick is to try to visualize what those chambers are doing in any given rhythm situation. Let’s see if a quick review of some strips helps the visualization process.
Here we are familiar Sinus rhythm on image 01. Organized, rhythmic, producing stable contraction of the chambers – first the atria, then the ventricles. So nice orderly motion, first above, then below.
 Image 01
Image 01 Next slide (Image ) atrial flutter. Still organized: the atria are contracting rapidly, sure, at about 300 bpm, and the ventricles are responding to every third or fourth impulse, slowly enough that the ventricular chambers have time to fill up nicely between beats, fast enough to probably maintain a good blood pressure. So I visualize the atria clipping along, with the ventricles contracting every third or fourth time.

Image 02
This one? Well – is it organized? Actually it is: see the pattern of doubles? It’s a little easier to figure out by looking at the lower part of the strip – this is a sinus rhythm, and after every sinus beat comes a PAC, followed by a compensatory pause. So yes, still organized. “Regularly irregular”.

Image 03 How about this one? , VT. Ugly, scary, but still organized, regular – the chambers (which ones?) are moving in a steady manner. On your mental screen you should see the ventricular walls contracting very rapidly – do they have time to fill? Should we shock this rhythm? It depends…

Image 04
1-1: What is atrial fibrillation
How about this one? Not organized? Should we shock this rhythm? A-fib for sure can be a shock able rhythm, but look at the QRS rate – in the 70’s. What would have to be happening to make this a shock able situation? What do you visualize here? Atria: bag of worms. Ventricles – occasional, but normally conducted QRS’s. Are they too slow or too fast to make a blood pressure? How do you tell?
 Image 05
Image 05 1-2: What is ventricular fibrillation?Here’s an ugly one - you probably recognize this one right off. Doesn’t look organized to me! What rhythm is this? Visualize the ventricles – everybody see the worms? What should we do?
 Image 06
Image 062- What is De-fibrillation?
So: all set on organized, and not organized? The treatment for nasty arrhythmia is often electrical, right? The point is: one type of treatment: cardioversion - is for the organized kind of rhythm, and the other is, De-fibrillation is for disorganized rhythms.
What you want to do is to send a fixed amount of electrical energy along the normal conduction path of the heart: along the Lead II pathway.
Image 07
Here’s a diagram of the normal lead II: the positive electrode is down near the apex of the ventricles, the negative one is at the atrial end. Everybody remembers that the normal direction that the cardiac impulse takes is from the SA node at the northwest corner, up near Oregon, down and towards the southeast in Florida, where the positive electrode lives? And that the signal moves along the pathway as the cells depolarize, in sequence, along that pathway?
2.0: What is a defibrillator.
2.1: The monitor.
you need to be able to see what’s going on. This is of course one of the
reasons why our patients are monitored at the bedside: so you can see
what rhythm your patient is in. Defibrillators are built to travel– so they
have a built in monitor screen.
2.3: The capacitor.
Generally you need a battery to run any transportable medical device.
Due to rechargeable batteries these devices are so heavy. The batterystores electricity,when machine is plugged in to AC. The capacitor fills
up with electricity when you push the button that selects charge .
2.4: The paddles and the pads:
Paddles
Self Adhesive Pads
paddles are considered “old-tech” – nowadays the thing to do is to slap on sticky defibrillation pads that hook up to the machine – the same ones as
external pacing pads – then stand back, charge and discharge the machine
from a few feet away. The shock can be delivered to the heart by means of
electrode placed on chest of the patient(External defibrillation) or the electrode
may be held directly against the heart when the chest is open
(internal defibrillation). Higher voltage are required for external defibrillation
than for internal defibrillation.
2.5: Theory of operation.
Schematic diagram of a defibrillator
Above schematic show basic circuit diagram of DC Defibrillator. A Variable auto transformer forms the primary of a high voltage transformer. The output voltage transformer is rectified by a diode rectifier and is connected to vacuum type high voltage change over switch. In position 1, the switch is connected to one end of an oil filled micro farad capacitor. In this position, the capacitor charge to a voltage set by the positioning of the auto transformer. When the shock is delivered to the patient, a foot switch or a push button mounted on the handle of the electrode is operated. The high voltage switch change over to position 2 and the capacitor is discharged across the heart through the electrode. The inductor in the circuit slow down the discharge from capacitor by induced counter voltage. This give the output pulse a physiologically favorable shape. The dis advantage of using inductor is that any practical inductor will have its own resistance and dissipates part of the energy during the discharge process. The shape of waveform that appears across electrodes will depend upon the value of the capacitor and inductor used in the circuit. The discharge resistance which the patient represent for defibrillating pulse may be regarded as purely ohmic resistance of 50-100 Ω approximately for typical electrode size of 80 cm2. The typical discharge pulse of defibrillator is shown in fig.3 b. Using this design, external defibrillation uses: –50 to 100 Joules of energy when electrodes are applied directly to the heart –Up to 400 Joules when applied externally ,Capacitors used range from 10 to 50F .Voltage using these capacitors and max energy (400J) ranges from 1 to 3 kV . Energy loss result in the delivery of less than theoretical energy to the heart
Defibrillator: Rectangular-Wave
•Capacitor is discharged through the subject by turning on a series silicon- controlled rectifier.
•When sufficient energy has been delivered to the subject, a shunt silicon- controlled rectifier short-circuits the capacitor and terminates the pulse, eliminating a long discharge tail of the waveform
•Output control can be obtained by varying:
–Voltage on the capacitor
–Duration of discharge
•Advantages of this design:
–Requires less peak current
–Requires no inductor
–Makes it possible to use physically smaller electrolytic capacitors
–Does not require relays ·
Monophasic pulse width is typically programmable from 3.0 to 12.0 msecBiphasic positive pulse width is typically programmable from 3.0 to 10.0 msec, while the negative pulse is from 1.0 to 10.0 msec ·
Studies suggest that biphasic pulses yield increased defibrillation efficacy with respect to Monophasic pulses.
Reference : http://coep.vlab.co.in
Ventricular Fibrillation
No comments:
Post a Comment